

STROKE
BRIDGE THE GAP TO YOUR DIAGNOSIS AND MANAGEMENT


Did you know this about strokes?
Stroke is a common occurrence, and can be permanently disabling. Most people recover from a stroke well, but depending on how severe it is. The majority of strokes are minor. However, a minor stroke or a transient ischaemic attack (a stroke-like event lasting <24 hours) may be the harbinger of a more disabling attack. Therefore, full appropriate investigation of any stroke-like event is important to address risk factors and initiate necessary treatments.
Most disabling and large strokes are due to rhythm abnormalities of the heart, especially atrial fibrillation. Most small strokes (which can be equally disabling) have no identifiable cause (cryptogenic). Reduction of the risk of a further disabling stroke can be achieved through use of antiplatelet drugs (Aspirin, Clopidogrel, Dipyridamole), anti-coagulation (only where indicated such as in Atrial Fibrillation), ceasing smoking, treating high blood pressure, improving diabetes control, treating high cholesterol, and other rarer contributing factors (e.g. Fabry’s disease).
Not all strokes are clots or blockages (~70%) because some are bleeds. Different types of bleeds can occur and identifying the cause of bleeding (blood vessel malformations, hypertension, cerebral amyloid angiopathy) helps to guide specific treatments. Bleeding is also seen after a clot has occurred, but treatment is aimed at treating the cause of the clot.
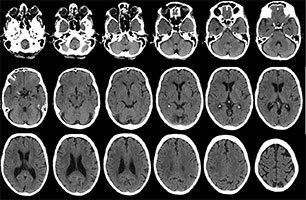
All suspected stroke should be neuroimaged, and, in the hyperacute phase, a CT scan is the most useful to make sure there isn't a bleed. CT early on can also identify clot and the changes associated with clot-related stroke to give emergency treatment such as thrombolysis (rtPA) or consideration of emerging treatments such as thrombectomy.
Once a stroke has happened, the ensuing disability may improve, stay the same, or sometimes worsen (due to complications of the stroke). Worsening usually happens in very disabling large clot-type strokes, or in bleeds.
There are many conditions that look like a stroke and in the emergency setting about half of all presentations of suspected stroke are mimics. The most common mimic is due to the headache disorder Migraine.
Migraine can cause paralysis, visual problems, speaking block (dysphasia), dizziness and vertigo. There may be little or no headache with these (migraine aura sine cephalgia). This type of presentation is common perimenopausally in women, and often occurs months/years before menopausal symptoms begin. There may be a family history of Hemiplegic Migraine. Other mimics include epileptic fits that are complicated by a transient post-seizure paralysis (Todd’s paresis), hypoglycaemia (usually Insulin overdose), and Wernicke’s encephalopathy (a B-vitamin deficiency disorder).
VIEW INFO ON MULTIPLE SCLEROSIS
Correct identification of the underlying presentation may be difficult as there may not be any investigation finding to go on, but a thorough history taking and examination by a specialist will usually help to identify a cause and therefore guide treatment.
